Aortic Dissection Stanford B. A case report
Keywords:
Aortic dissection; Angio-TAC; Chest pain; Mortality.Abstract
Introduction: chest pain is a common presentation in the emergency department environment. Although most cases of chest pain that present in the emergency department are eventually diagnosed as non-cardiovascular aetiology, it is important to exclude acute life-threatening conditions such as acute myocardial infarction, pulmonary embolism, visceral perforation and aortic dissection. This publication aims to show the importance of CT Angiography in the diagnosis of this disease and to review the updated bibliography.
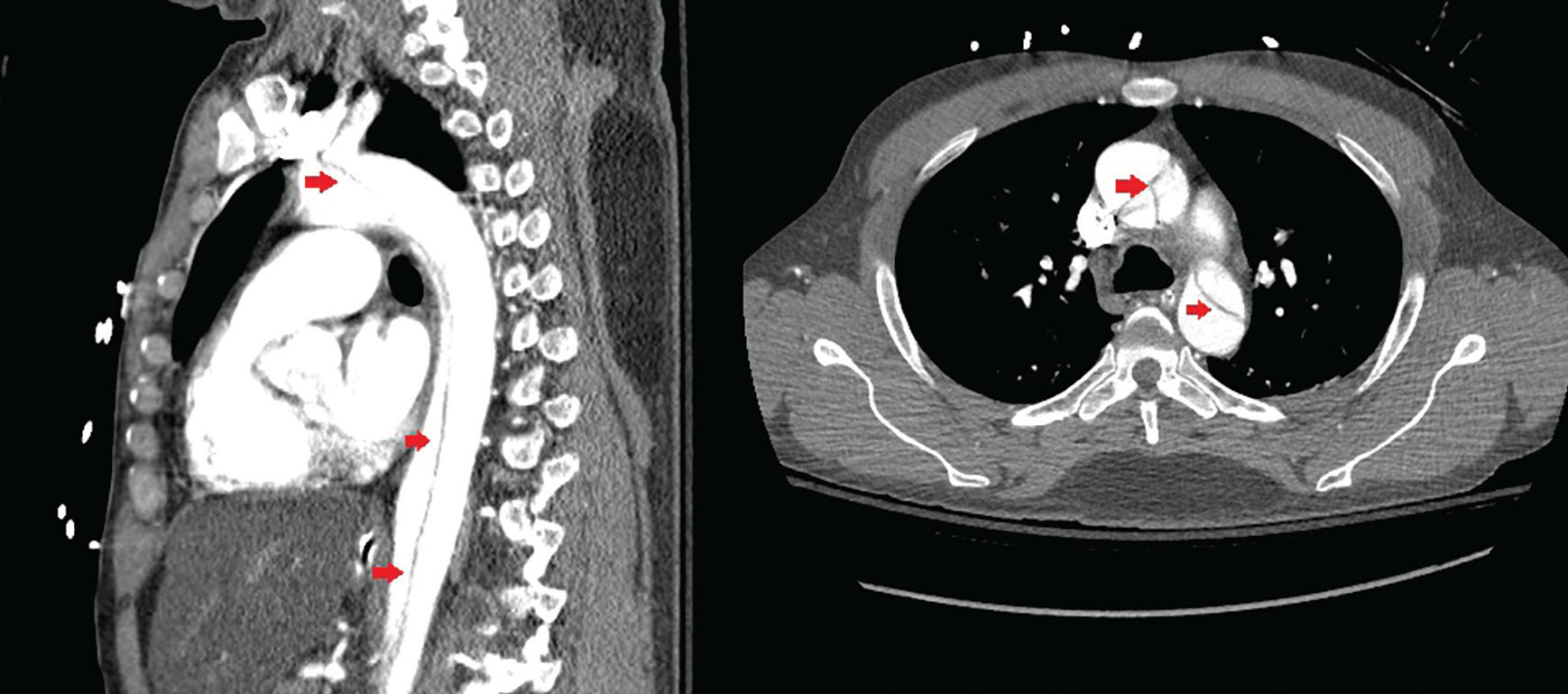
Case presentation: 45-year-old male patient with onset of chest pain and arterial hypertension, on CT angiography.
Discussion: a type B aortic dissection was performed according to Stanford and type III according to the DeBakey classification, the patient was stabilized, cared for by a cardiologist, and referred to a tertiary hospital. Aortic dissection is a disease to consider in young patients who complain of sudden chest pain, hypertension, mainly if the D-dimer is altered;
Conclusions: aortic dissection is a disease with a high risk of mortality that must be treated early; the most important radiological study in the diagnosis is CT angiography, the most common clinical presentation is atypical chest pain.
Downloads
References
1. Al’Aref SJ, Giraldi NL, Lau C, Devereux RB, Ghosh BD, Swaminathan RV, et al. A Contemporary Review of Acute Aortic Dissection. Emergency Medicine 2015; 5(5): 274.
2. DeMartino RR, Sen I, Huang Y, Bower TC, Oderich CS, Pochettino A, et al. Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality from 1995 to 2015. Cir Cardiovasc Qual Outcomes 2018; 11(8): e004689.
3. Gawinecka J, Schonrath F, Eckardstein A. Acute aortic dissection: pathogenesis, risk factors, and diagnosis. Swiss Med Wkly 2017; 147: w14489.
4. Fukoi T. Management of acute aortic dissection and thoracic aortic rupture. Journal of Intensive Care [Internet]. 2018 [Citado 4/1/2020]; 6(15). Disponible en: https://doi.org/10.1186/s40560-018-0287-7
5. Lempel JK, Ann Frazier A, Jeudy J, Kligerman SJ, Schultz R, Ninalowo HA, et al. Aortic Arch Dissection: A Controversy of Classification. Radiology 2014; 271(3): 848-55.
6. Chishti MA, Rawat V, Nagarwal P. Acute Dissection of the Ascending Aorta: A Case Report and Topic Review. Journal of Mahatma Gandhi University of Medical Sciences and Technology 2017; 2(1): 31-34.
7. Vululi ST, Rwebembera J, Openy AB, Bugeza S. Atypical Clinical Presentation of Extensive Aortic Dissection at Mulago Hospital: Case Report. J Thrombo Cir [Internet]. 2018 [citado 2/1/2020]; 4(2). Disponible en: https://www.longdom.org/open-access/a-typical-clinical-presentation-of-extensive-aortic-dissection-at-mulagohospital-case-report-2572-9462-1000126.pdf
8. Lei P, Jun Hong Y, Fu Quan G, Gong L, Sha Sha H, Guo Hong C, et al. Case report of a 28-year-old man with aortic dissection and pulmonary shadow due to granulomatosis with polyangiitis. BMC Pulmonary Medicine [Internet]. 2019 [citado 2/1/2020]; 19(122). Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6615146/
Downloads
Published
How to Cite
Issue
Section
License
Avisos de derechos de autor propuestos por Creative Commons
1. Política propuesta para revistas que ofrecen acceso abierto
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:- Los autores/as conservarán sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cuál estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación esta revista.
- Los autores/as podrán adoptar otros acuerdos de licencia no exclusiva de distribución de la versión de la obra publicada (p. ej.: depositarla en un archivo telemático institucional o publicarla en un volumen monográfico) siempre que se indique la publicación inicial en esta revista.
- Se permite y recomienda a los autores/as difundir su obra a través de Internet (p. ej.: en archivos telemáticos institucionales o en su página web) antes y durante el proceso de envío, lo cual puede producir intercambios interesantes y aumentar las citas de la obra publicada. (Véase El efecto del acceso abierto).